
CEC2024 | 张玮教授:II型内漏--EVAR30年唯一无解之并发症

2024年10月31日—11月3日,备受瞩目的第十五届中国血管论坛(CEC2024)于北京盛大召开,国内外专家齐聚一堂共襄盛会。本次大会设置知名专家面对面、中青年专家论坛、学术专题讲座,病例直(录)播、外周血管介入前沿与争锋辩论赛、疑难病例大查房、复杂血管疾病、血管外科危重症管理、血管疾病治疗并发症处理及预防、外周器械新技术新疗法、下肢动脉减容规范化应用最新证据深度解读、国际专场@CEC等热点板块,全面展现最新的血管疾病诊疗方法和技术,为广大血管外科医务工作者及同道提供了一场内容丰富、高质量、高水平的学术盛宴。
本次大会期间,首都医科大学附属北京安贞医院 张玮教授为各位专家同道介绍了《Type II Endoleaks Following EVAR:A problem with no resolution for 30 years》。欢迎阅读。
演讲题目:
《Type II Endoleaks Following EVAR:A problem with no resolution for 30 years》
演讲嘉宾:
张玮教授
单位:
首都医科大学附属北京安贞医院

临床背景与核心问题
疾病现状
主动脉瘤腔内修复术开展 30 年,一型、三型内漏已有成熟方案,四型内漏少见
二型内漏仍未妥善解决,单纯器械改革无突破,临床处理棘手
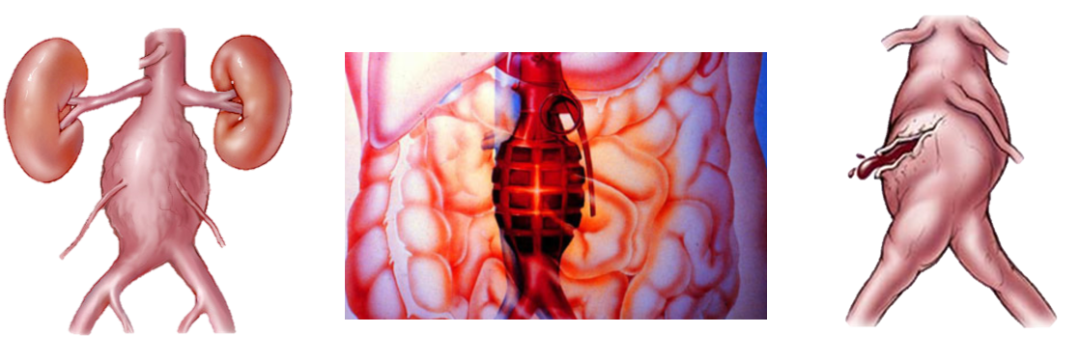
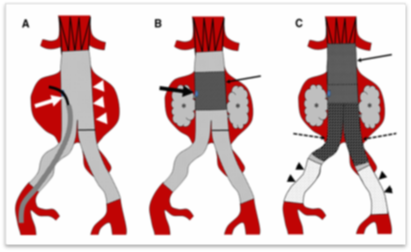
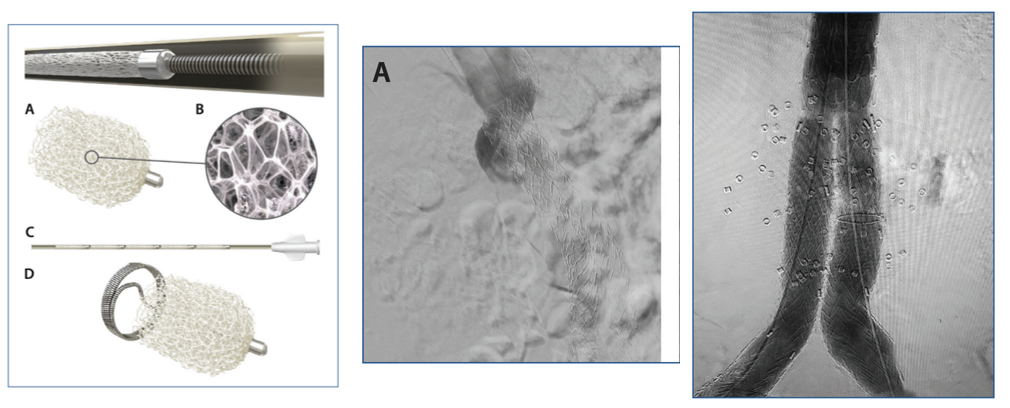
治疗手段
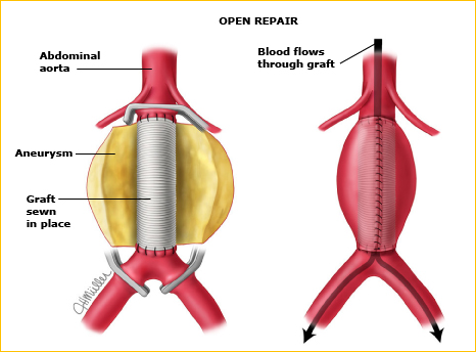
图为:开放修复术
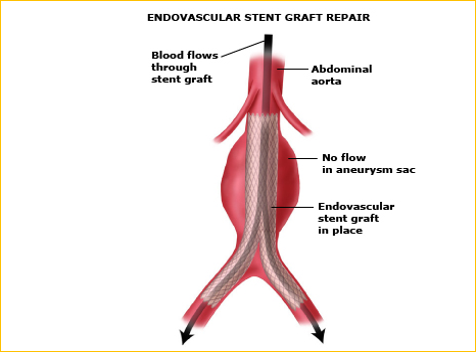
图为:血管内支架移植物修复
内漏的分类
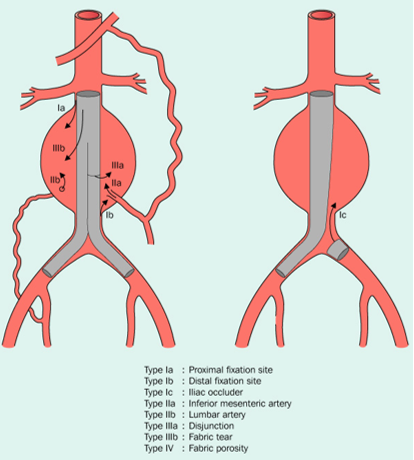
Type I: attachment site
Ia: proximal
Ib: distal
Ic: iliac occluder
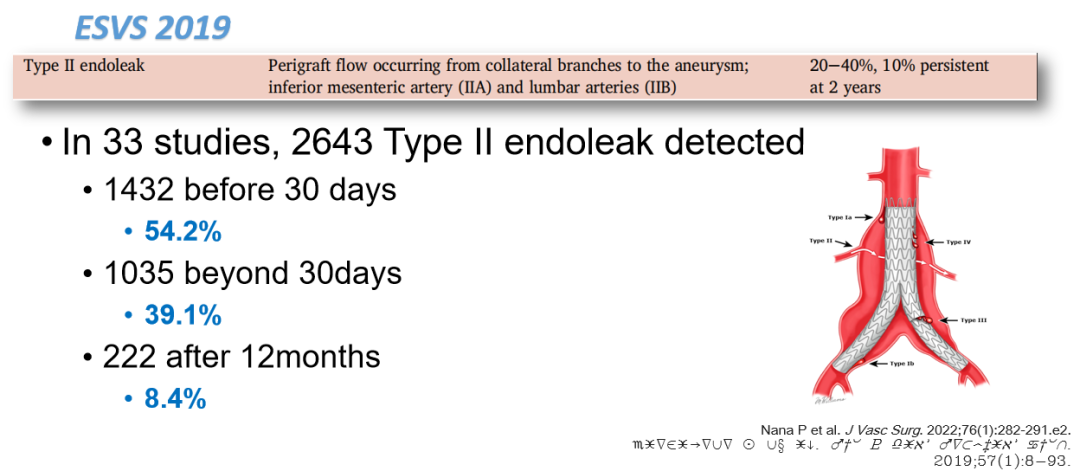
Type II: collateral vessel
IIa: IMA
IIb: Other Branches
Type III: failure of graft
IIIa: disjunction or fracture
IIIb: fabric tear
Type IV: fabric porosity
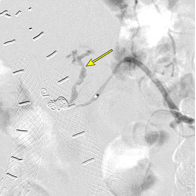
II型内漏
II型内漏的发生率
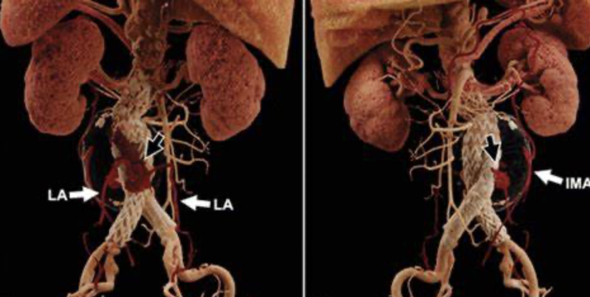
II型内漏的原因
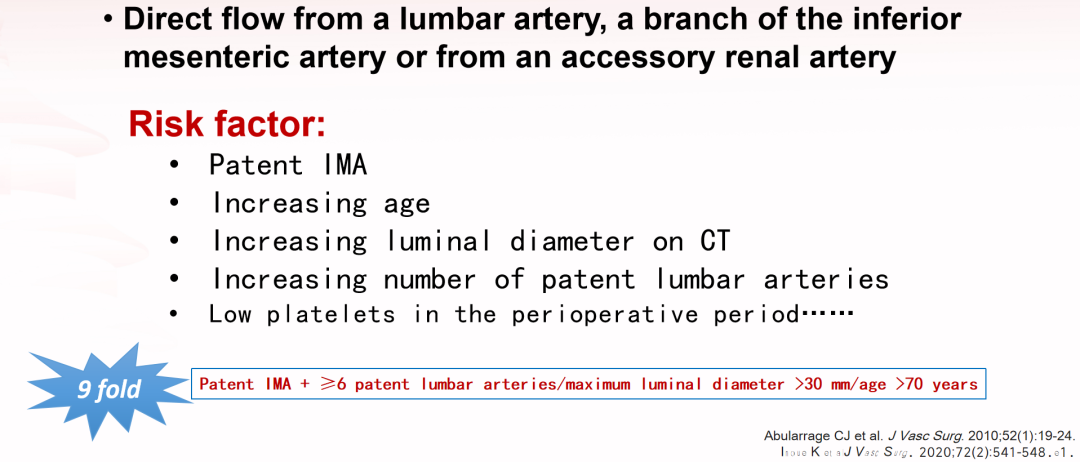
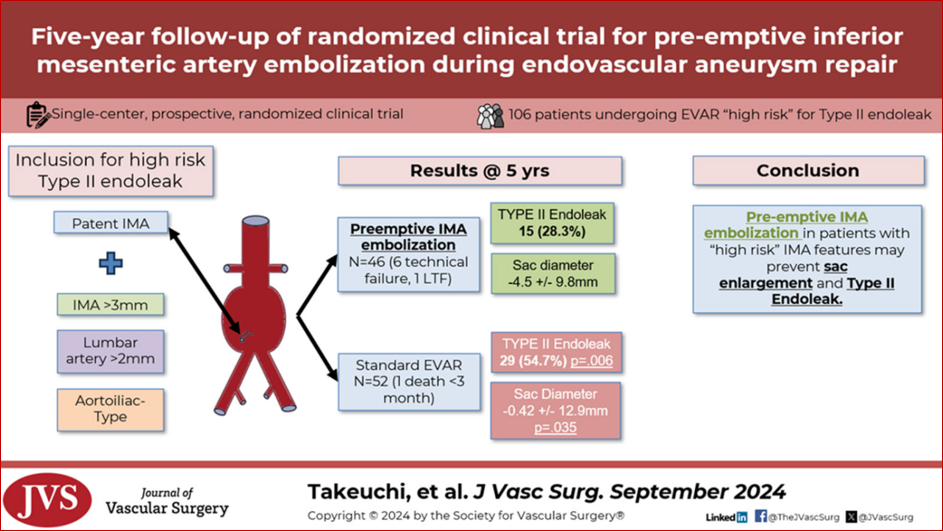
危险因素
肠系膜下动脉(IMA)>3mm、腰动脉>2mm
动脉瘤累及髂动脉(尤其髂总、髂内动脉),瘤囊直径>6.5cm
年龄、抗凝 / 抗板治疗史
IMA ≥3 mm in diameter
lumbar arteries ≥2 mm in diameter
an aortoiliac-type aneurysm
Aneurysm >6.5cm
II型内漏的后果
Persistent Type II endoleak can lead to:
Aneurysm sac growth
Device migration
Component separation
Open conversion
Rupture
The aneurysmal sac increased in 29% persistent Type II endoleaks.
Nine studies reported 14 ruptures
Rate of 1.1% (0% to 5.3%)

诊疗指南与干预手段
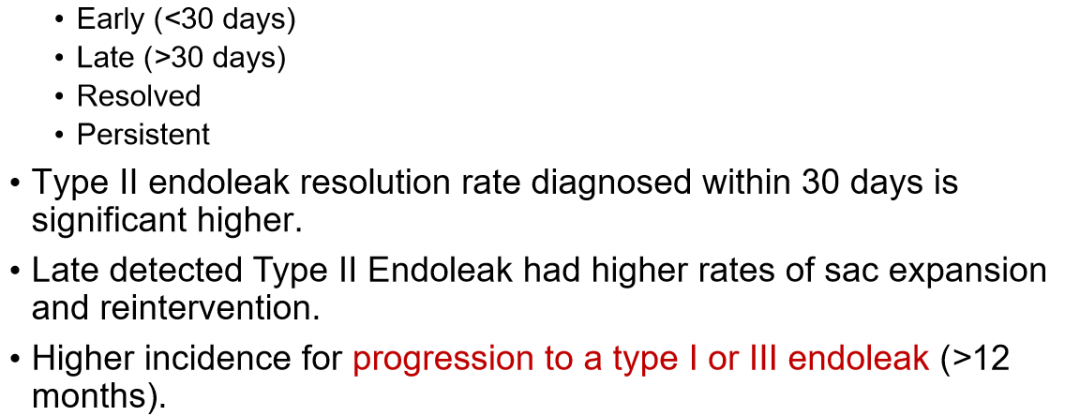
随访显现

long term follow-up whenever detected
Three-phase CTA at regular time, especially for patients with sac expansion.
Duplex US if no sac expansion
预防
干预指征
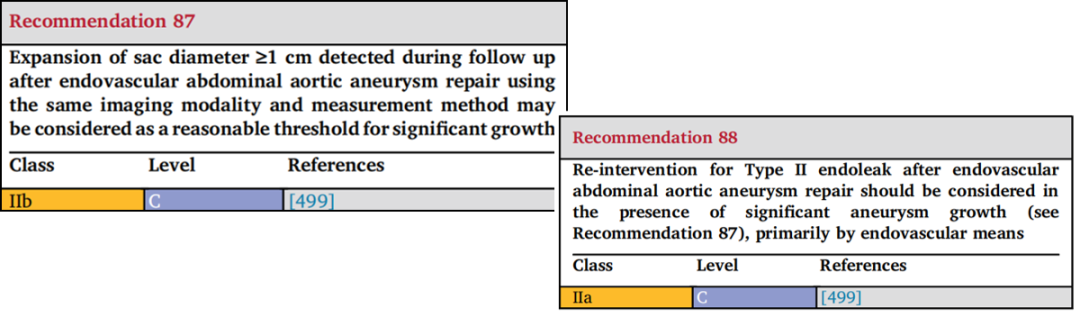
ESVS:aneurysm sac expansion ≥1 cm(level C)
欧洲指南:术后瘤囊扩大超 1cm 需干预
SVS: aneurysm sac expansion ≥5 mm(level C)
美国 SVS 指南:随访中瘤囊直径超 5mm 需干预
Other proposed criteria:
Endoleak persistence >6 months
Presence of large nidus
More than three feeding or draining arteries
Feeding artery diameter >4 mm
High-flow velocities in aneurysm sac
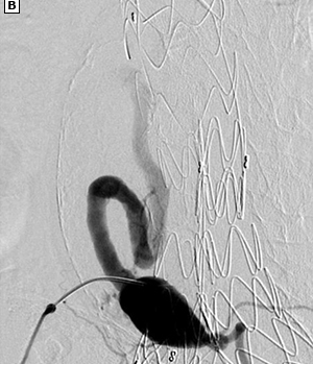
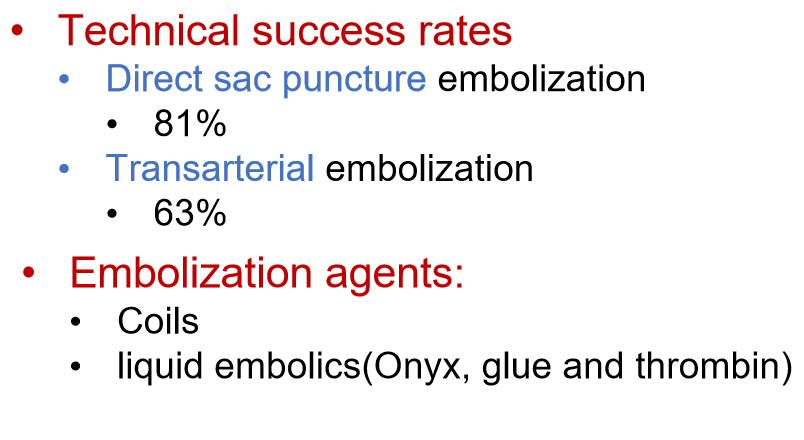
干预与预防手段

Aneurysmal sac embolization
Trans-vessel Approach
Transcaval
Transarterial perigraft
Transarterial transgraft
Direct Sac Puncture Approaches
Percutaneous translumbar
Percutaneous transcaval
Percutaneous transabdominal


临床挑战与展望
Type II endoleak associated with AAA expansion >1cm
Treatment is recommended.
Type II endoleaks with no AAA enlargement
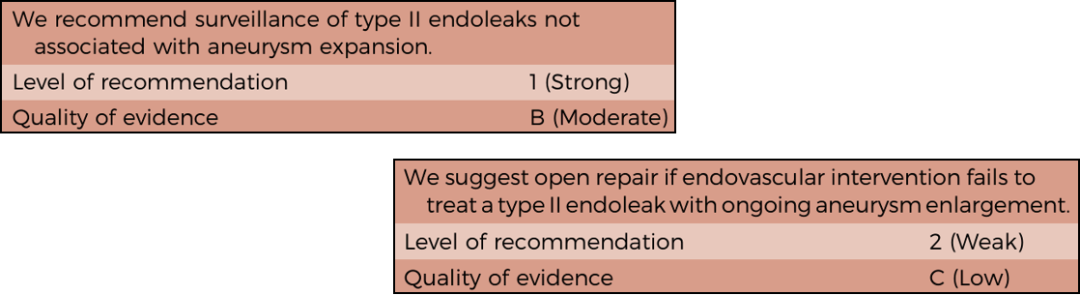
Surveillance
Endovascular re-intervention is the first choice
Conversion to open surgical repair is recommended if a Type II endoleak does not resolve with endovascular treatment.
未来展望
We need a stentgraft to prevent Type II endoleak at the time of EVAR without extra procedures
专家介绍

张玮教授
首都医科大学附属
北京安贞医院
血管外科首席专家
首都医学科学创新中心特聘研究员、心血管疾病独立研究室主任
首都医科大学讲席教授,血管外科学系主任
清华大学杰出访问教授
华盛顿大学医学院临床教授
美国血管外科学会杰出会员
美国Annals of Vascular Surgery《血管外科年鉴》、共同主编
《血管外科年鉴:创新报道》杂志总编辑
《中华血管外科杂志》副主编